MAY 2026
Featured Research / Findings
HPV Vaccination Coverage in Italy
A Nationally Guaranteed Prevention Strategy
Human papillomavirus (HPV) vaccination is one of the key preventive interventions included in Italy’s Essential Levels of Care (LEA), ensuring equal and free access for all eligible cohorts. The national program targets girls and boys aged 11 (twelfth year of life) through active invitation, with extended free catch-up coverage up to age 25 for females and 18 for males; in some Regions, free access is further expanded for females up to 30 years. Monitoring of vaccination uptake is essential to evaluate equity, identify geographical gaps, and assess the program’s capacity to protect future adult cohorts from HPV-related cancers.
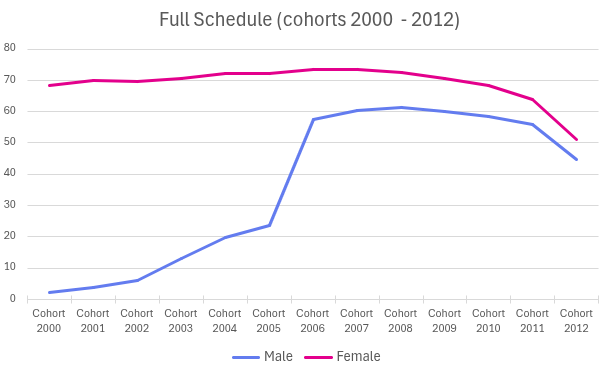
This report presents national and regional HPV vaccination coverage as of 31 December 2024, focusing on females and males born between 2000 and 2012. Data were collected through the annual reporting system coordinated by the Ministry of Health and the Regions.
HPV Vaccination Coverage in 2024: Overall Overview
Female Cohorts (2000–2012)
Coverage levels among females remain higher than among males, reflecting longer program implementation and earlier introduction. National coverage with:
- ≥1 dose: ranges from 66.29% (cohort 2012) to 75–80% in older cohorts,
- Cohort: ranges from 51.18% (cohort 2012) to over 74% in some Regions and cohorts.
Younger cohorts, still engaged in active invitation, show lower completion rates but are expected to increase as cycle completion progresses.
Regional variability:
- Best-performing Regions: Umbria, Emilia-Romagna, Tuscany, Lombardia consistently record ≥80% first-dose coverage in mid and older cohorts.
- Lowest coverage: Sicilia, Calabria, Campania show persistent gaps, with full schedule coverage often below 50%.
Older female cohorts (2000–2004) show the cumulative effect of prolonged catch-up strategies, with completion rates around 70%.
Male Cohorts (2000-2012)
Male coverage remains substantially lower than female coverage in older cohorts, due both to the later introduction of routine vaccination for males and to cultural factors. Since 2007, vaccination was actively offered only to 12-years-old girls, with the campaign being extended to boys from the 2017 onwards.
Key national findings:
- Cohorts 2012–2010: Coverage significantly improved, reaching 64–66% for ≥1 dose and 45–58% for completion.
- Cohorts 2009–2007: Uptake increases to around 66–68% for ≥1 dose while remaining stable for the completion.
- Cohorts 2006–2000: Coverage dramatically declines, with many Regions reporting <10% for ≥1 dose—reflecting limited historical catch-up adherence.
Regional differences are larger for males:
- Northern Regions (Veneto, Emilia-Romagna, Friuli-Venezia Giulia) consistently report ≥70% in younger cohorts.
- Southern Regions (Campania, Sicilia, Calabria) fall well below national averages (often <40%).
- Significant anomalies: exceptional high male coverage in Puglia for several cohorts (up to ~78%), indicating effective regional engagement strategies (school involvement).
Geographical Inequalities
HPV vaccination coverage in Italy remains strong in many Regions, particularly in the North and Centre, but significant geographical and sex-related disparities persist. Younger cohorts, especially boys, show encouraging progress, while older cohorts reveal the consequences of delayed introduction and limited historic catch-up coverage.
Future objectives
Improving equity remains the central priority. Strengthening outreach, reinforcing active-call systems, and integrating HPV vaccination with broader adolescent health strategies will be essential to ensure nationwide protection against HPV-related diseases.
Authors
Subscribe to our newsletter to get news and updates.
![]()
Views and opinions expressed are however those of the author(s) only and do not necessarily reflect those of the European Union or European Health and Digital Executive Agency (HaDEA). Neither the European Union nor HaDEA can be held responsible for them.
This website is managed by 6th DYPEDE, Greece.





This project has received funding from the European Union’s EU4HEALTH Programme under the Grant Agreement no 101162959